What Really Ails Us? – Part II Patient Monitoring: Finding Trouble Early
September / October 2005
What Really Ails Us?
Part II Patient Monitoring: Finding Trouble Early
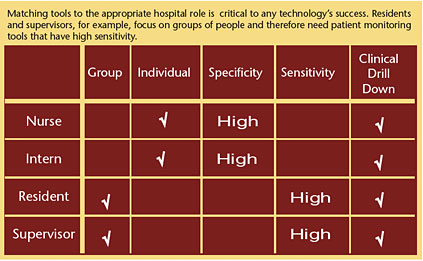
Nurses and interns need high specificity alerts: if the alarms goes off, it’s likely to be significant. Residents and supervisors need high sensitivity alerts: the alarm catches events that, if ignored, could develop into a failure to rescue.
In What Really Ails Us? Part I: Failure to Rescue and Errors of Omission (PSQH), July/August 2005, I looked at the root causes of failure-to-rescue and came to some fundamental conclusions:
- Errors of omission-errors that occur as a result of a step not taken or when an appropriate step is left out from a process-are the primary cause of preventable hospital mortality.

- We lack a systematic way to handle clinical decompensation, and we can’t get the performance levels that patients need by relying on a paper medical record.
- To achieve better outcomes, we need to electronically enable rapid response teams and supervisorial staff.
In fact, technology has the potential to enable patient care performance levels that cannot be achieved any other way. A simplistic view is that caregivers should receive an alert whenever something dangerous happens. However, while alerting has been around for many years, there are some fundamental misunderstandings about how to get the most value from them.
Alerting Misses the Mark
Alerting has most often been targeted at bedside caregivers (physicians, nurses, interns) with the display of information or a warning in the middle of a task, such as CPOE, or as a disruption, intended to signal the occurrence of a significant event. The rationale for the former is that the alert represents information caregivers did not already have, and in the latter example, that as clinicians receive alerts, they can drop what they’re doing, rush off to investigate the problem, and solve it. Sounds good, but in practice it has been a dismal failure.
In both cases, the predominant limiting factor has been the eventual development of “alert fatigue.” Bedside caregivers inevitably ignore alerts because most alerts highlight events that they already knew about or considered inconsequential. The response to this dilemma has been either to turn off the alerting altogether or to send alerts only for extreme conditions, which leads us back to where we started.
Alerting fails under these conditions because hands-on caregivers are task-oriented. They are focused on individual patients and have a long list of tasks to complete during their shift: talk to patients, write orders, draw blood, write notes, check results, and so on.
Alerts break the train of thought and interrupt workflow and often inform the caregiver of data that has already become known in the course of normal diligent care.
But, as the old saying goes, you don’t throw the baby out with the bathwater. In other words, alerting isn’t the problem. The way alerting tools have been targeted is the problem. We can preserve alerting to caregivers about truly critical situations, but alerting tools are more successful when one considers the needs of those in supervisorial roles.
Current failure-to-rescue statistics measure the efficacy of traditional methods of problem identification and resolution, suggesting there is substantial room for improvement.
Match the Tool to the Role
Unlike caregivers, supervisors (charge nurses, residents, respiratory therapy supervisors) are tasked with looking at a larger group of people and seeing the
big picture view in order to match resources to need. Supervisors have the responsibility to provide a safety net and have the time to look for trouble spots in the hospital and intervene to ensure optimal care.
Those responding to problems need to be able to scan the horizon for problems and be able to drill down for details. Alerting tools, calibrated to have high sensitivity, can give that broad perspective, which suits supervisorial roles.
Matching tools to the appropriate hospital role is critical to any technology’s success. As hospitals continue to set up rapid response teams, supervisors can effectively create a safety net, backstopping the sometimes overwhelmed hands-on caregivers. Yet, to avoid overwhelming supervisors and the rapid response team with high sensitivity alerts, hospitals need to make sure that they are given patient monitoring tools that help them work smarter, not harder.
Display Must Help Identify Trends
Effective patient monitoring tools need to incorporate display features that convey information about alerts in a useful, effective manner. Presenting alerts for each aberrant clinical value could quickly prove confusing and counter-productive. Indeed, a change in a clinical condition can be expected to produce changes in a variety of related clinical indicators.
But, when aberrancies are grouped, patterns become more evident without losing the essential clinical information. For example, the respiratory category includes respiratory rate, oximetry, inspired oxygen concentration, and blood gas data. The infection category includes WBC count and temperature. Rather than seeing a series of individual values, a clinician seeing several respiratory alerts in combination with several infection alerts could be expected to have a high index of suspicion of respiratory infection or sepsis.
Having identified a patient with abnormal values, supervisors must be able to quickly drill down and formulate a synthesis of the patient’s clinical condition based on the data.
Toggling between a display screen that shows the hospital big picture and screens that show the patient’s clinical big picture can be a very effective way to identify patients most in need of intervention by supervisors or the rapid response team.
Another way to combine discrete data elements to identify patients with specific circumstances is to use any of several scoring systems. This methodology assigns a different number of points for each of several clinical variables, with the number of points reflecting the degree of variance from normal values. Examples include SNAP (Score for Neonatal Acute Physiology) (Richardson, et al., 1993) and MEWS (Modified Early Warning Score).
According to Subbe et al. (2001), a reliable score can be calculated by describing and validating MEWS, by considering multiple variables (blood pressure, heart rate, respiratory rate, temperature, and a simple mental status score). The higher the score, the more likely the patient will end up in trouble.
Absolute elevations indicate a higher risk for a bad clinical outcome, and rising scores are likely to be even more significant. As the nurse enters the values, the severity score is calculated automatically and displayed. The caregiver gets the benefit of seeing the aggregate score and uses this to validate the clinical impression or to heighten the level of concern.
At the supervisor level, a quick scan of the hospital-wide view shows where the sickest patients are located. Some obvious mismatches between needs and resources are often evident, e.g., a patient with breathing problems on a floor that rarely cares for such patients, suggesting a possible expertise deficiency. Or, there may be a larger than usual number of patients with severe problems, which suggests the potential for a staffing deficiency.
By immediately drilling down into individual patient data, those values that caused the alerts are evident and other integrated views of data present a coherent picture of the patient’s clinical status and recent course. By sequentially applying this method to many patients, staff can find those most likely to be in trouble and proceed further with an in-person evaluation.
Patient Monitoring for Early Intervention
As noted in Part I, rapid response teams are now seen as an effective strategy for finding and treating patients early. The ideal composition of the rapid response team is still being investigated. Some teams draw on existing roles, such as supervisors. Regardless, supervisors and rapid response teams will be more effective if they have technology assisting their efforts at early detection and response.
Patient monitoring technology is a critical aspect of any rapid response team because it:
- Highlights patients needing special focus
- Presents data in a format that enhances trend recognition
- Facilitates expeditious evaluation of patients’ clinical condition
In addition to watching patients for immediate problems, patient monitoring tools present a whole new view of patients and how to manage them.
Sharp Healthcare, based in San Diego, California, is using patient monitoring tools to improve diabetes outcomes. Diabetes case managers use the technology to evaluate patients identified by the monitor as having a blood glucose value outside the acceptable range. At any given moment, a case manager can see which patients need top priority intervention.
This is worth noting because these are interventions with patients admitted for other conditions. By using patient monitoring tools, hospitals can now proactively scan their patients for the development of complications that could result in failure-to-rescue if left for delayed intervention.
Summary
With a renewed focus on patient safety, it’s critical that patient monitoring technology not only become part of any rapid response team, but that these tools also get in the hands of hospital staff charged with assessing a larger group of patients.
It’s not enough to simply have electronic monitoring and alerting. If the information isn’t given to the right people and if the data isn’t displayed in a meaningful way, patient safety will not improve significantly.
Richard Kremsdorf (richk@clinicomp.com) is CEO and president of CliniComp, International in San Diego, CA, which develops clinician documentation systems for hospitals, integrated delivery networks, academic medical centers and other acute care providers. Formerly, Kremsdorf served as vice president, clinical information systems, at Catholic Healthcare West, a 48-hospital system, and as medical director of clinical information systems at ScrippsHealth. Most recently, he was CEO of Five Rights Consulting. He is an experienced speaker and educator and wrote the landmark publication Medication Safety Tools 2001-3, which defined the essential capabilities of CPOE and electronic medication administration. Kremsdorf is a graduate of Massachusetts Institute of Technology and Albert Einstein College of Medicine and serves as a member of the Editorial Advisory Board for PSQH.
References
Richardson, D. K., Phibbs, C. S., Gray, J.E., McCormick, M.C., Workman-Daniels, K., & Goldman, D. A. (1993). Score for neonatal acute physiology: A physiologic severity index for neonatal intensive care. Pediatrics 91,617-23.
Subbe, C. P., Kruger, M., Rutherford, P., & Gemmel, L. (2001). Validation of a modified early warning score in medical adminssions. QMJ 94, 521-526