Rapid Response Teams: Clinical Triggers and Rapid Response Escalation Criteria
March / April 2007
Rapid Response Teams
Clinical Triggers and Rapid Response Escalation Criteria
Previous studies have demonstrated that hospitalized patients often experience significant adverse events during their hospital stays because of the hospital staff’s failure to recognize or respond to early signs of clinical deterioration (Devita, et al., 2006). As a result thereof, rapid response teams (RRT) have been popularized. The goal of these teams is to respond with alacrity to inpatient staff who are concerned about a patient, before physiologic deterioration is so advanced so as to preclude successful intervention. The members of the RRT vary by hospital but often include an intensive care unit (ICU) physician and nurse, along with a respiratory therapist. This concept is predicated on the truism that patients often have physiological deterioration several hours before they become unstable or suffer a cardiopulmonary arrest (Hillman, et al., 2001).
Notwithstanding the increasing deployment of these teams in hospitals, the evidence supporting broad implementation of RRTs is at best tenuous (Winters, Pham, & Pronovost, 2006; Esmonde, et al., 2006). Therefore, given the fact that at Denver Health we have in-house residents and interns 24 hours a day, 7 days a week, we decided to institute a variation on the RRT that better suited our needs and would avail a timely and thorough assessment and plan for patients who are starting to deteriorate.
The specifics of our program are as follows: If a nurse notes that her patient’s clinical condition is worsening, she is asked to quickly determine if any one of certain “clinical triggers” are present. These include:
- a respiratory rate less than 8 or greater than 28;

- an acute change in oxygen saturation less than 90% despite oxygen administration;
- threatened airway;
- acute change in systolic blood pressure to less than 90mmHg or a sustained increase in diastolic BP greater than 110mmHg;
- acute change in heart rate less than 50 or greater than 120 beats per minute;
- new onset chest pain;
- an acutely cold, cyanotic, or pulse-less extremity;
- confusion, agitation, or delirium;
- unexplained lethargy;
- difficulty speaking;
- acute change in pupillary response;
- new seizure;
- temperature greater than 39.0 Celsius;
- uncontrolled pain;
- acute change in urine output less than 50ml/4 hours; or
- acute bleeding.
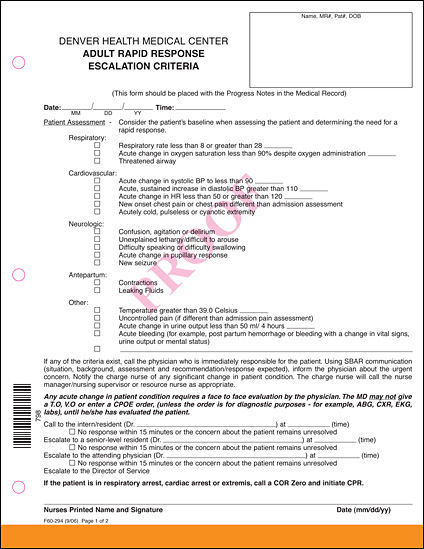
If any of these criteria exist, the nurse is required to call the physician who is immediately responsible for the patient. Using structured communication (SBAR: situation, background, assessment, and response expected), the nurse informs the resident about the urgent concern and that this is an “adult rapid response clinical trigger” call.
Any call for a clinical trigger issue mandates a face-to-face evaluation by said physician. The doctor may not give a telephone or verbal order, or even enter a computerized provider order entry (CPOE) order, until he or she has evaluated the patient. Orders for diagnostic purposes such as a blood gas, chest radiograph, or electrocardiogram (EKG) are permitted.
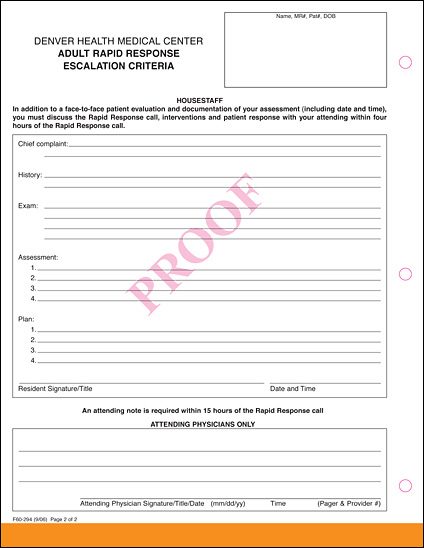
If the initial physician contacted does not respond within 15 minutes or the concern about the patient remains unresolved, the expectation is that the nurse will escalate her concern to a senior resident, the attending physician, or even to the director of service, if there continues to be no response. The nurse is required to fill out the Adult Rapid Response form as is the responding physician and his or her attending physician. The resident must discuss the intervention and patient’s response with the attending physician within hours of the rapid response call.
The advantages of this system are many. First, it averts the confusion of involving a brand-new team that may have no prior knowledge of the patient’s clinical status. Second, it averts “handoffs,” which is important because it is known that such handoffs beget an opportunity for errors. Third, it promotes empowerment of nursing staff and familiarity with structured communication, which often impacts patient safety (Christian, et al., 2006). Finally, the costs of standard RRT programs may be significant and can be avoided with this program.
While we do not yet have formal evidence that our approach is a better one, it is clear that educational efforts to help staff better recognize deteriorating patients earlier is beneficial (Buist & Bellomo, 2004). The Denver Health “Clinical Trigger — Adult Rapid Response” program is inextricably connected with a need for clinical acumen to recognize deteriorating patients. Currently, the RRT concept has, at best, only relatively weak evidence supporting its efficacy and thus may not be the panacea needed to negate a failure to rescue deteriorating patients (Wachter & Pronovost, 2006).
Philip Mehler was born in Denver, Colorado, and went to medical school at the University of Colorado. After completing a residency and chief residency in internal medicine, he joined Denver Health, Colorado’s public safety net hospital, in 1987. From 1993 to 2003, he was the chief of internal medicine, and in 2003 he was promoted to associate medical director and director of patient safety and quality. His research interests include hypertension control, cardiac risk modification, and the medical complications of anorexia and bulimia. He has authored more than 200 pieces of scholarly work and is a professor of medicine at the University of Colorado where he holds an endowed chair. From a patient safety and quality standpoint, his main focus is in the areas of hypertension and diabetes control, reducing failure to rescue occurrences and nosocomial infections, and on-time occurrence reporting. Mehler may be contacted at pmehler@dhha.org.
Kendra Moldenhauer graduated from the School of Nursing at the University of Northern Colorado in 1983 and joined Denver Health as a staff nurse in 1984. She was the nurse manager for the outpatient surgical specialty clinics and adult critical care and the trauma program manager for the Level I trauma center at Denver Health Medical Center. Moldenhauer is currently the manager of patient safety and quality.
Allison Sabel is the director of medical biostatistics at Denver Health. She is a board-certified preventive medicine physician. She completed an MPH in epidemiology before entering a MD/PhD program at Tulane University with her PhD in biostatistics. Sabel was chief resident of both her transitional residency and preventive residency programs. She has taught biostatistics for 10 years at the graduate school level at Tulane University and University of Colorado. Sabel is currently on faculty in the Department of Preventive Medicine and Biometry at the University of Colorado Health Sciences Center.
References
Buist, M. & Bellomo, R. (2004). The emergency medicine team or the medical education team? Critical Care Resuscitation, 6, 88-91.
Christian, C. K., Gustafson, M. L., Roth, E. M., Sheridan, T. B., Gandhi, T. K., et al. (2006). A prospective study of patient safety in the operating room. Surgery, 139, 159-173.
Devita, M. A., Bellomo, R., Hillman, K., Killum, J., Rotondia, A., et al. (2006). Findings of the first consensus conference on medical emergency team. Critical Care Medicine, 34, 2463-2478.
Esmonde, L., McDonnell, A., Ball, C., Waskett, C., Morgan, R., et al. (2006). Investigating the effectiveness of critical care outreach services: a systematic review. Intensive Care Medicine, 232, 1713-1721.
Hillman, K. M., Bristow, P. J., Chey, T., Daffum, K., Jacques, T., et al. (2001). Antecedents to hospital deaths. Internal Medicine Journal, 31, 343-348.
Wachter, R. M. & Pronovost, P. J. (2006). The 100,000 lives campaign: A scientific and policy review. Joint Commission Journal on Quality and Patient Safety, 32, 621-627.
Winters, B. D., Pham, J., & Pronovost ,P. J. (2006). Rapid response teams — Walk, don’t run. Journal of the American Medical Association, 296, 1645-1647.