Minnesota State Coalition Works to Prevent Violence Against Healthcare Workers
Implementation and dissemination
In July 2014, the coalition asked the CEOs of all healthcare facilities in Minnesota to participate in a pilot campaign in which they would commit to make workplace violence prevention a top priority by:
- Completing the Prevention of Violence in Healthcare gap analysis
- Supporting the development of (or continued work on) a violence prevention committee in their organization
- Participating in educational webinars on workplace violence
- Completing a survey after nine months to share progress and continued needs
More than 100 facilities signed on to the campaign. The majority of participating facilities were hospitals, but surgery centers, long-term care facilities, and homecare organizations also joined.
Results
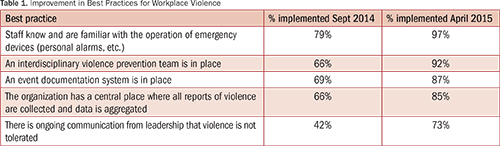
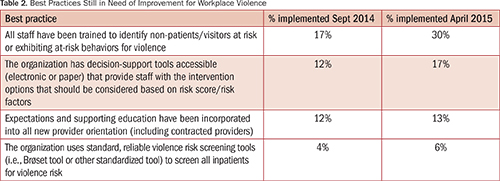
Initially, facilities worked to complete the gap analysis and then implemented best practices to fill identified gaps in policies and procedures. After nine months, the coalition asked participating facilities to update their gap analysis. Strong improvement was seen in a number of areas during the pilot (Table 1). Organizations also identified a number of areas where gaps remained, though these metrics also showed modest improvement during the pilot (Table 2).
Discussion
Minnesota’s experience with workplace violence prevention has provided a number of key lessons about how to develop and implement process changes within and across organizations, as well as the sometimes hidden barriers to change in a multi-stakeholder collaborative. These lessons offer insight for organizations just beginning their journeys to prevent and respond to violence against staff:
Support from leadership is vital.
As with any culture change, the change needs to be led and supported by leadership at all levels and spread throughout the organization. Successful organizations in Minnesota have senior leaders who have established from the beginning that violence against staff will not be tolerated. In addition, those organizations provide resources in the form of time and money to address these issues on an ongoing basis.
Organizations must have a centralized system for collecting reported events and a process for learning from them.
Prior to this campaign, most organizations had some form of incident reporting system in place. However, not many had a system where all incidents of violence were reported or aggregated into one central location. Many organizations send some reports to employee health, some to security, and still others to human resources, preventing any single department from seeing the true scope of the issue. Finding a way to collect reports in a central location has proven to be crucial for success. Only after all incidents are aggregated and analyzed can organizations see the full scope of the problem, identify patterns and trends, learn from the occurrences, and put practices in place to prevent them from happening again.
Organizations need to change the staff’s acceptance of a culture of violence.
Even though it is a major cultural shift, senior leaders of organizations need to work to change their staff’s perception that violence is an accepted part of the job. Some organizations use in-person meetings, newsletters, and emails to continually remind staff to report these events for further learning. Ongoing communication via multiple modalities ensures staff members know that violence is not an accepted part of the job and that leadership is actively working to prevent incidents from occurring and learning from them when they do occur.
Relationships with local law enforcement are crucial.
For violence prevention and response plans to be most effective, organizations should establish a relationship with law enforcement proactively, not during an emergency. Successful organizations make local law enforcement members of their violence prevention teams, leverage their expertise for training and education, and keep them engaged in their facility’s processes and plans.
Minnesota’s Violence Against Health Care Workers Law
Recognizing the importance of this issue and foundational work done by the coalition, the 2015 Minnesota legislature passed a law that requires all hospitals in the state to:
- Designate a committee of healthcare workers to develop preparedness and incident response action plans for acts of violence.
- Review their action plans at least annually.
- Make action plans available to local law enforcement and, as appropriate, to collective bargaining units.
- Provide training to all healthcare workers employed or contracted with the hospital on safety during acts of violence, both annually and upon hire. Training must include, at a minimum:
– Safety guidelines for response to and de-escalation of an act of violence
– Ways to identify potentially violent or abusive situations
– The hospital’s incident response reaction plan and violence prevention plan
- As part of its annual review, the hospital must review with the designated committee:
– The effectiveness of its action plans
– The most recent gap analysis
– The number of acts of violence that occurred in the hospital during the previous year, as well as injuries that occurred
The law also includes penalties; the Commissioner of Health may impose an administrative fine on a hospital for failure to comply with the requirements of this law.
Many organizations had already voluntarily adopted some or all of the strategies outlined in the violence prevention gap analysis as part of the Coalition’s voluntary pilot, including establishing multidisciplinary teams. The law sets clear expectations that build on that work and offers an opportunity to assist organizations in providing training to all staff, forming and maintaining a violence prevention committee, and developing and implementing plans to prevent and respond to incidents of violence so that both patients and staff are safe.
Conclusion
The Prevention of Violence in Health Care Coalition will continue to help guide this work as the requirements of the new law are implemented. A number of next steps will assist with advancing prevention and response in Minnesota:
- MDH solidified a formal alliance with the Minnesota Occupational Safety and Health Administration and developed a no-cost video training for hospitals to help them meet the requirements of the law. The training module is now available online for use. It is also exploring ways to partner with the Veterans Administration to share training materials and other resources.
- A number of organizations have indicated that the only standardized, validated risk assessment tool currently available (Brøset Violence Checklist) is validated exclusively for use in inpatient psychiatric units. The Coalition, therefore, is investigating the possibility of validating a tool for statewide use or developing a new tool that facilities can use in other settings or units across the continuum of care.
- In response to challenges that some hospitals experience in identifying training or educational options appropriate for their workforce, the coalition has developed a clearinghouse of materials in addition to its recorded training modules.
- The Coalition will continue to explore ways to support organizations that are not subject to the law’s requirements but where violence is also a known issue, such as long-term or postacute care facilities and clinics.
Minnesota has a long history of multi-stakeholder and multidisciplinary collaboration on many important health quality and patient safety issues. This work is another example of the positive difference statewide partnerships can make. With these steps, Minnesota is positioned to significantly improve safety and security at healthcare facilities for employees, patients, and visitors, and to create a culture in which violence is no longer accepted as part of daily life for healthcare professionals.
Rachel Jokela is director of the adverse health events program at the Minnesota Department of Health and may be contacted at Rachel.Jokela@state.mn.us.
Diane Rydrych is director of the Health Policy Division at the Minnesota Department of Health.
Tania Daniels is vice president of quality and patient safety at the Minnesota Hospital Association.
Rahul Koranne is chief medical officer at the Minnesota Hospital Association.
References
Gomaa, A. E., Tapp, L. C., Luckhaupt, S. E., Vanoli, K., Sarmiento, R. F., Raudabaugh, W. M., … Sprigg, S. M. (2015, April 24). Occupational traumatic injuries among workers in health care facilities — United States, 2012–2014. Morbidity and Mortality Weekly Report, 64(15), 405–410. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6415a2.htm
U.S. Bureau of Labor Statistics (2013). Survey of Occupational Injuries and Illnesses, 2013. Retrieved from http://www.bls.gov/respondents/iif/forms/soii2013.pdf