Event Reporting: How Rhode Island Is Leading a Revolution in Patient Safety
January/February 2011
Event Reporting
How Rhode Island Is Leading a Revolution in Patient Safety
This is the first in a series of articles about the statewide implementation of a standardized web-based event-reporting platform to facilitate the reduction of medical errors.
Rhode Island has played a leadership role in a number of revolutions throughout history. It was the first of the original 13 colonies to declare independence from Great Britain, igniting the American Revolution. Years later, the construction of the first successful textile mill in Pawtucket, Rhode Island, signaled the start of the Industrial Revolution in the United States.
Today, Rhode Island continues that trailblazing tradition by leading efforts in another critical area: patient safety. Thanks to a statewide initiative to standardize the reporting and analysis of both adverse and near-miss medical events, Rhode Island will unite its private acute care hospitals—technologically and culturally—in a common effort to reduce medical errors.
From Sanctions to Solutions
Medical error is well documented in medical journals and commands increasing attention by providers, government, and the public. The federal government has launched major initiatives to reduce medical error and improve patient safety while regulators in Rhode Island are working collaboratively with providers to address this important issue.
A series of wrong site surgeries in Rhode Island was the catalyst for the creation of a statewide committee representing surgeons, operating room directors and regulators, to look at ways to ensure a safer environment for patients at all Rhode Island hospitals.
The Hospital Association of Rhode Island (HARI), an advocacy organization for hospitals, co-led the initiative with William Cioffi, MD, surgeon-in-chief at Rhode Island Hospital. Hospitals in the Ocean State have demonstrated a continued commitment—to improving the safety and quality of patient care. Past accomplishments have included statewide adoption of a uniform surgical protocol and creation of the Rhode Island ICU Collaborative, an initiative that has successfully reduced the incidence of infections in critical care units.
Because of these past successes and their commitment to quality patient care, the chief executive officers (CEOs) of hospitals across the state readily agreed to have their organizations participate in a new project to standardize medical event reporting. An executive steering committee was formed with representatives from HARI and hospitals, including chief nursing officers (CNOs), quality/risk managers, and IT personnel.
A Critical Need for Standardized Reporting
The key issue for the executive steering committee was transparency—improving the way data on adverse events was being reported, analyzed, shared and utilized to reduce patient harm. Another important goal was to encourage hospitals to foster an environment for open dialogue and improve care by learning from the experiences of peers. Implementation of the standardized reporting tool is well underway, with hospitals reporting a significant increase in reported events, including near-miss events that did not result in injury or patient harm but had the potential to do so (no-harm events). With the early and systematic identification of trends, health care providers will gain insight into safety problems, providing knowledge that will ultimately lead to improved processes for patient care at all hospitals in Rhode Island.
A critical component in achieving transparency on a statewide scale was to have all hospitals implement the same medical event-reporting technology and standardize their reporting criteria. At that time, the hospitals used a variety of manual and electronic methods to track events. Also, event definitions, questions asked, and data analysis methods differed widely from institution to institution. Even if hospitals were to find a way to share data with one another, there would be no common ground for analysis and interpretation.
Having a standardized reporting platform was important for another reason. Rhode Island was in the process of creating a state-certified patient safety organization (PSO). A PSO is a protected central repository that enables healthcare providers to report data on adverse and near-miss events without fear of discovery. This “safe harbor” environment encourages the sharing of information within the PSO so institutions can uncover and correct the systemic factors that undermine patient safety. In order for the PSO to be effective, a standardized event-reporting system that could be used by all hospitals to populate the repository was needed.
Technology to Drive Compliance and Accountability
The executive steering committee assessed a number of vendors and associated event-reporting systems and selected the Medical Event Reporting System (MERS) from GE Healthcare. This web-based system met three key criteria: it is easy to use so hospital personnel would be more likely to enter and analyze data, improving compliance based on a variety of criteria, its routing function sends reports immediately and automatically to managers and administrators, improving accountability and speed of follow-up; and its color-coded, real-time dashboard gives managers clear visibility into the status of each event inquiry, improving communication.
Knowing that technology alone would not solve the standardization challenge, the executive steering committee looked at other factors in the selection process. The fact that the GE Healthcare MERS team included quality, safety, and change management experts who would be available to support and guide the hospitals through the process of implementation and employee adoption of the MERS system was also critical to the selection. Five performance-improvement consultants and four implementation specialists from GE Healthcare worked with HARI and the hospitals as did Harold S. Kaplan, MD, and Barbara Rabin Fastman, MHA, MT (ASCP) SC, BB, two of the clinical content developers of the MERS software.
Statewide Structure
A seminal decision made by the hospitals early on was to develop a statewide steering committee consisting of the CNOs from each of the hospitals and co-chaired by a CNO from one of the hospitals and leadership from HARI. In most hospitals, patient safety is the responsibility of quality control and/or risk management departments. Quality and risk managers typically have no operational responsibilities—they can examine problems and suggest action but have limited authority to take action. The hospitals believed structuring the steering committee so that operational owners provided statewide guidance and had ownership for program implementation at the hospital level was critical. This approach would secure the involvement of clinical owners who had the experience, insights, and authority to make operational improvements across the greatest number of patient care areas in the hospital.
The first hurdle for the statewide steering committee was to gain consensus on standardization of the inputs to MERS and definitions of patient safety terms. Successful implementation of the MERS technology depended on getting all of the hospitals to agree on hundreds of standardized definitions for event-reporting categories, from pharmacy services and medication safety to falls, infection control, and general patient care events. The hospitals also had to define what constituted an adverse event versus a near-miss in order to capture outright process failures as well as early warnings that if not caught, could lead to patient harm. The change management and facilitation skills provided by the GE Healthcare team were particularly critical to the success of this phase of the project.
Benefits Emerge Early
Project teams were formed at each hospital to contribute to the standardization effort and to oversee implementation at the individual institutions (Figure 1, pg. 35). The teams came together in five working sessions between March and July 2010 to reach consensus on the definitions and forms for data input into MERS. These half-day and full-day meetings were facilitated by the GE and MERS consultants and typically involved more than 50 participants from across the state. The project teams consulted prior to these meetings with their subject matter experts in order to be prepared to provide feedback during the general working sessions. In certain circumstances, the subject matter experts were also invited to the working sessions when it was clear that gaining consensus was dependent on having these experts in the room. The next article in this series will take readers inside these sessions and show how the team was able to achieve consensus and create an event-reporting platform that met the goals of the Rhode Island initiative as well as the individual requirements of each hospital.
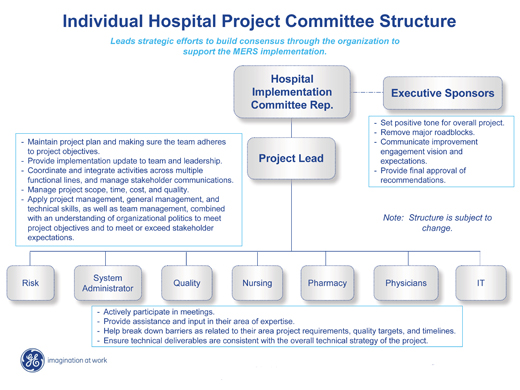
Figure 1. Individual Hospital Project Committee Structure
(click here to view a larger version in a separate window)
As the standardization effort progressed, clear benefits were emerging for the hospitals even before the final work was completed:
- Better communication. The process improved communication channels among the hospitals that were limited prior to this initiative.
- Shared learning. By arriving at a common language to talk about patient safety and track events, the hospitals were able to share information and learn from one another more quickly and effectively.
- Accelerated implementation. Implementing an event reporting system is a challenging task. When a hospital tackles such a project on its own, decisions often get deferred due to uncertainty and ambiguity, and the process can easily become sidetracked. Rhode Island’s group initiative used a structured approach, a detailed timeline, and peer encouragement to force timely decision-making and drive rapid implementation.
- Peace of mind. It’s estimated that more than two-thirds of hospitals in the United States do not have established environments that support medical event reporting. A major impediment is uncertainty over data protection issues. Many hospitals are not reporting adverse and near-miss events because they are unclear about the regulations surrounding data reporting. Through the statewide effort, the individual hospitals in Rhode Island were given access to expert resources with knowledge and experience around these issues, giving them a greater sense of security about their participation.
In the next article, we will not only share insights on how to gain consensus across multiple hospitals but also what it means to be a part of a statewide PSO. We look forward to wrapping up 2011 by sharing the outcomes from this initiative and providing a template for others across the country that are interested in developing a state or regional coalition.
Joanne Dooley is vice president and chief nursing officer at Roger Williams Medical Center in Providence, Rhode Island.
Jean Marie Rocha is vice president for clinical affairs at the Hospital Association of Rhode Island in Cranston, Rhode Island.
Patricia Daughenbaugh is senior manager at GE Healthcare Performance Solutions.
Kathy Martin is director of the GE Healthcare Patient Safety Organization. She may be contacted at Kathleen.Martin@med.ge.com.