Don’t (Always) Give Blood
November/December 2013
![]()
Don’t (Always) Give Blood
A Team-Oriented Approach to Reducing Bodily Harm in Cardiac Surgery
Every Friday morning at Abington Memorial Hospital in suburban Philadelphia, cardiac surgeons, anesthesiologists, medical technologists, and critical care nurses gather to discuss new protocols. Later the same day, they go on rounds together, gathering at open-heart surgery patients’ bedsides to share knowledge and look for ways to improve outcomes for these critically ill patients.
The main topic is blood. Specifically, this team is working to reduce the use of donor blood, which is now seen by many patient safety advocates in a new light as a result of recent research (Koch et al., 2006). Clinicians at Abington want their patients to come out of open-heart surgery without the bloated, ashen look typically seen after exposure to heart-lung machines and an excessive volume of fluid in their bodies. And they want these patients to go home sooner to resume healthy, productive lives.
We came to Abington in 2010, along with a team of clinicians from SpecialtyCare, an international company that runs the hospital’s perfusion services—the heart-lung machines that support cardiovascular function during cardiac surgery. We had worked together previously at several top Philadelphia teaching hospitals, including the Hospital of the University of Pennsylvania and Hahnemann University Hospital. Each of us had been a part of implementing some data-based best practices in blood management at other hospitals.
At Abington, we saw an ideal opportunity to do a comprehensive program, as the use of blood and blood components was above national averages. Senior hospital leadership was on board with our efforts, and we had buy-in from the other cardiothoracic surgeon, Mauricio J. Garrido, MD. The size of the staff was small enough to overcome the inertia of prior practice. We pursued a team approach, with anesthesiologists, perfusionists, and critical care nurses asked to play key roles.
The project included mechanical changes to the heart-lung machine designed to minimize the need for blood transfusions and reduce post-surgical complications. It also involved a number of protocol changes in post-operative care designed to ensure that patients aren’t hemodiluted—a condition that occurs when the fluid content of the blood increases, lowering the concentration of red blood cells and clot-forming proteins.
Our overarching goal was to reduce donor blood transfusions. Until fairly recently, blood and blood products—red blood cells that carry oxygen to tissue and take away carbon dioxide; plasma, a fluid that contains proteins that help the blood clot to avoid bleeding; and platelets, cell fragments that interact with proteins to prevent bleeding—were thought to be wholly beneficial for patients. Blood, after all, is the essence of life, and once donors were screened and blood was properly typed, handled, and stored, giving blood was seen as a safe and routine medical intervention.
A Liquid Organ Transplant
Although there is no doubt that donor blood is of life-saving importance in care for accident victims, cancer patients, and others, it is also far from a benign substance.
Research over the past few years by Colleen Koch, MD, cardiac surgery anesthesiologist at Cleveland Clinic, and colleagues has helped raise concern about the overuse of transfusions (Koch et al., 2006). A large study published in Critical Care Medicine in 2006 and based on more than 10,000 coronary artery bypass operations at the clinic, found significantly higher rates of death, kidney failure, heart attacks, surgical-incision infections, post-operative bleeding, significantly longer hospital lengths of stay, and other complications among transfused patients compared with those who didn’t receive blood (Figure 1).
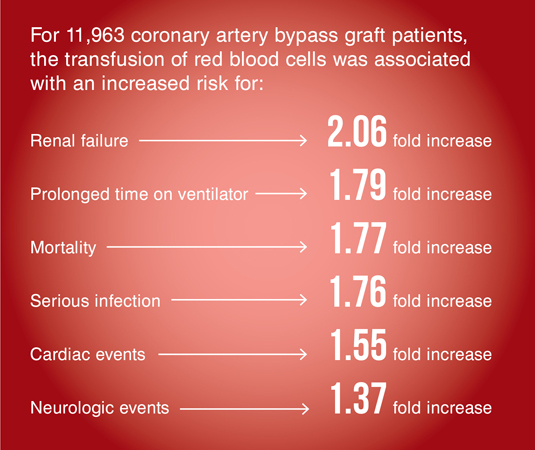
Figure 1. The Risk of Transfusions
Source: “Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting,” Critical Care Medicine, June 2006
Administering banked donor blood is essentially a liquid organ transplant. Through that transplant, the recipient’s own immune system is altered for some period of time. In addition, 60 or more human interactions must occur for a patient to receive a unit of blood. The human events begin from the moment that blood is collected from a donor or that a patient has his or her blood drawn for blood typing until it is infused into a recipient. Human error in this scenario can include mislabeling, contamination, using the wrong unit, or confusing one patient’s blood sample with another’s.
Donor blood transfusion improves outcomes in only 11% of clinical scenarios for patients without trauma or active bleeding, according to research published in 2011 by the International Consensus Conference on Transfusion Outcomes, a group of clinical experts in the fields of anesthesiology, intensive care, hematology, oncology, surgery, and patient blood management (Shander et al. 2011,).
This work and research in Europe and Brazil in recent years has led to a new movement in medicine: patient blood management. The Society for the Advancement of Blood Management defines it as “the timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration, optimize hemostasis and minimize blood loss in an effort to improve patient outcome.”
Despite this nascent effort, current practice generally is decidedly not based on clinical evidence or protocols. A study led by Elliott Bennett-Guerrero, a researcher at Duke University’s Duke Clinical Research Institute, found wide variation in transfusion practices at 798 U.S. hospitals, involving 100,000 people who underwent coronary-artery bypass surgery in 2008 (Bennett-Guerrero et al., 2010). Some hospitals gave transfusions to fewer than 10% of their patients, while other hospitals’ transfusion rates topped 90%. Researchers found that only about 20% of the variation was explained by how sick the patients were. They also found there wasn’t any link between a hospital’s use of transfusions and death rates.
Transfusions are given most commonly to correct serious anemia by boosting a patient’s hemoglobin, or red blood cell count. Normal hemoglobin ranges from about 13 to 18 grams per deciliter of blood in men and 12 to 15 grams in women.
Guidelines published by the Society of Thoracic Surgeons say that when hemoglobin is 6 grams or less, equivalent to a red-blood-cell level below 18%, transfusions can be life saving. When hemoglobin is more than 10 grams, or 30%, a transfusion is hardly ever beneficial.
Blood Use on the Rise
How much blood to give is also an issue. Patients are routinely given two units of red blood cells when one might be sufficient. Frankly, there is a lot of folklore around blood. Clinicians who would order the minimum effective dose of any other medication automatically order two units of blood. It isn’t based on clinical evidence; it is just what people have always done.
The result is a lot of blood being used. From 1997 to 2007, the number of discharged hospital patients who had received red blood cells doubled from 5% to 10.4%, with blood transfusion becoming the most common inpatient hospital procedure. Some 14.6 million units of blood are transfused annually, while 17 million units are donated.
All this transfusing comes at a staggering cost. A study in the April 2010 issue of Transfusion, a peer-reviewed academic journal, shows that when all of the complex cost factors are considered—including administrative, lab work, and labor—transfusing a single unit of red blood cells costs from $522 to $1,183, perhaps four times higher than previously thought (Shander et al., 2010).
Limiting Blood Use in Cardiac Surgery at Abington
It was in this context that we embarked on our program at Abington. We knew we could help achieve the Triple Aim of higher-quality, more cost-effective, and safer patient care by adopting a series of best practices.
Blood management in cardiac surgery is of particular importance. These procedures historically involved a lot of transfusions, a result of the invasiveness of the procedure and the nature of the technology.
Heart surgery is dangerous, mainly because of the risks associated with the heart-lung machine. We decided to turn the tables: instead of fearing this machine, why not treat it like an ally in our effort to get the patient back from surgery looking like he did before surgery, instead of appearing to be 20 pounds heavier as a result of excess fluid? Why not have patients go home sooner, in four or five days instead of seven?
And why not have the patient spend less time on a ventilator and in the cardiac care unit with its one-to-one nurse-to-patient ratio?
Exposing blood to the surfaces within the heart-lung machine provokes an inflammatory response that can damage red blood cells. The patient can dilate and lose fluid from blood vessels to tissue and outside the body. To reduce intravascular depletion, the patient receives additional volume at the risk of hemodilution.
Furthermore, the heart-lung pump must be primed (to remove air in the tubing) with a solution that also maintains sufficient blood volume between the machine and the patient for survival during surgery. The downside is that this fluid also dilutes the patient’s blood, often to the point where needed blood components, including clot-forming proteins, are less effective, meaning the patient bleeds excessively and can become acutely anemic.
By minimizing the size of the circuit to which the blood is exposed, the need for donor blood transfusions is significantly reduced.
The heart-lung machine carries blood from the right atrium of the heart to a main reservoir called a cardiotomy, which uses an oxygenator that keeps the red blood cells oxygen-rich. The blood cells then travel to an arterial filter that removes any hazards before the blood travels through a plastic tube back to the patient’s aorta.
The technical or mechanical changes undertaken at Abington were to raise the oxygenator and cardiotomy to the level of the patient, thus reducing the length of the circuit through which blood had to follow. The team then began using vacuum assist instead of gravity to bring blood more quickly from the patient to the machine, reducing time that the blood spends in the tubing.
A hemoconcentrator was added to the circuit that the blood passes through. This device removes plasma water—the fluid that separates red blood cells, platelets, and clotting factors—so we could retain a higher concentration of those products during the bypass run. Once the patient comes off bypass, the remainder of the volume left in the circuit is ultrafiltrated and returned to the patient via transfusion, often before patient leaves the operating room. Thus the patient gets back all of their own blood components.
Another goal of having patients retain their own blood components is to reduce bleeding at the surgical site and through chest tubes.
A Sense of Team
What we have done at Abington is implement best practices in blood management, but they are not common practices. They require teamwork, and every member of the team must work a bit harder. Perfusionists, anesthesiologists, and first assistant nurses need to be actively working to not give the patient blood.
Importantly, the regular Friday meetings allowed us to spread the word about our program to cardiologists and other physicians. One problem we encountered in the process was pushback from cardiologists, who would see readings of anemia in post-op tests and see an immediate need for transfusions. In short, this is often a “false anemia”; the patients actually have sufficient stores of essential blood components, despite the post-op readings.
It took cardiologists some time to see enough data to convince them that anemia was not physiologically significant and that patients recovered hemoglobin quickly without transfusion.
Meanwhile, we also made a change to protocol so that the patient would stay under the cardiac surgeon’s care for the first couple of days post-surgery, again to ensure no unnecessary transfusions occurred.
John Lanzidelle, president of operations for SpecialtyCare’s Greater Delaware Valley Region, thinks the teamwork involved from the operating room to the ICU to the cardiac care unit to the med/surg room was the most important element of Abington’s blood management project. “Before, there was no single set of guidelines that coordinated blood management during the patient’s entire stay; without the increased focus on blood management to improve patient care, blood might be ordered without considering all the potential consequences of giving that blood.”
Results
The results of the work at Abington are notable from both a quality of care and financial perspective, one of many small victories in the effort to improve the delivery of healthcare in the age of reform.
Comparing the first 9 months of 2010 with the same period in 2012:
- The average rate of transfusion decreased by 22%.
- Average amount of red blood cells transfused per case decreased by .98 units.
- There was an average per-case reduction of $3,500 cost for blood and blood component use; annualized savings of $1.05 million.
- The average postoperative length of hospital stay decreased by .61 days.
Furthermore, using fewer units of red blood cells led to better patient outcomes, such as lower incidence of acute kidney injury (Figure 2).
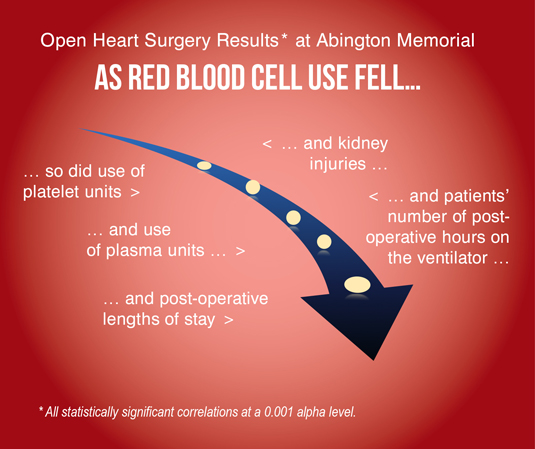
Figure 2. Reduced Blood Use, Better Outcomes: Open Heart Surgery Results* at Abington Memorial
Sources: SpecialtyCare, Abington Memorial Hospital
Most importantly, after surgery our patients look better, feel better, get well faster, and get back on their feet more quickly.
Blood is a life-saving resource, but our experiences and those of other institutions have shown that when it is safe to avoid using it, patients and organizations benefit. By avoiding unnecessary transfusions, more blood and blood products are available to those who truly need them, and the resources now devoted to excess blood use can be put to better use in improving patient care.
Rohinton Morris is chief of cardiothoracic surgery and the Porter Institute for Valvular Heart Disease at Abington Memorial Hospital in Abington, Pennsylvania. He received his MD from Hahnemann University School of Medicine in Philadelphia, where he also did a fellowship in cardiothoracic surgery. He is board certified in thoracic surgery. He can be reached at rmorris@amh.org.
Charles Yarnall is a national clinical specialist with SpecialtyCare (www.specialtycare.net), a Nashville, Tennessee-based provider of outsourced clinical services, including perfusion in open-heart surgeries. He is board certified in cardiovascular perfusion by the American Board of Cardiovascular Perfusion. He received his degree in cardiac perfusion from Allegheny University Hahnemann Division, School of Health Sciences and Humanities. He can be reached at charles.yarnall@specialtycare.net.
References