Community Circles: Transforming Care in Downeast Maine
These resources helped me galvanize EHC’s community-based, volunteer board of directors: In January 2011, they embraced the Four Agreements as a model to support their governance role. The EHC Table of Organization was revised with job titles that supported the evolving leaders as they implemented the tenets of the Four Agreements. Active feedback, brainstorming, and providing data were welcomed at all levels of the organization, ushering in a culture of transparency.
The first Community Circle, which convened in March 2011, was announced in the local newspaper as well as in the patient waiting room, and staff and board members, along with a local reporter, were invited to attend. Acknowledging that EHC’s change in leadership and providers had been disruptive to the community, the Circle’s goal was to engage citizens in recruiting providers and responding to the community’s healthcare needs. Several community members attended, and EHC sought direct input and feedback regarding their experiences at the health center. Two attendees were recruited to serve on EHC’s board. All present embraced the idea of attentive, responsive listening and a culture shift toward transparency.
The Circle’s success exceeded my expectations. Noting the United States’ move toward transformative healthcare change, I surmised that the Circle’s engagement model could be used to facilitate conversations and perhaps even support change in our local healthcare delivery system.
The Community Circle process
Community Circles use an open agenda with a defined aim and probing questions to facilitate active discussion. They also allow for silence. Circles honor all contributions and allow the conversation to flow where it needs to go. Sometimes the discussion moves to a whole new topic. In my experience, discussion comes back in a renewed way to the defined aim. Always, I am amazed how Circles uncover the complexity of the system or problem being discussed. This often occurs over time, through a series of Circles. Responsive listening allows well-considered ideas to surface, ones that can be tested as part of a solution. If participants bring up a topic that cannot be changed or reversed, responsive listening helps them to let it go. It allows a new tapestry to be woven.
In Eastport, we have used the Community Circle model of engagement for many conversations and topics: hospice care, the patient-centered medical home model, teens helping teens, understanding Alzheimer’s disease, community cancer resources, palliative caregivers, health and wellness, food insecurity, strategic planning, governance and leadership training, and others. Many Circles conclude after the initial conversation; others continue for several months, and still others meet regularly for years. Since March 2011, EHC has convened 92 Community Circles. The model has also been adapted to accommodate other EHC innovations, including Cultural Immersion Downeast, a one-week experiential program for graduate students that aims to help them appreciate the rich culture of the community in which they will practice. Of the 22 students who have completed this program, 10 have come back to Washington County for clinical rotations, and two have long-range plans to move here. Community Circles promote relationships!
We have developed and implemented local training for Community Circle participation. Eighty recipients across industry and community sectors have received training, and many have gone on to work with:
- Founders of innovative programs, such as the Maine Health Access Foundation
- Associations and coalitions, including Sunrise Health Care Coalition, five FQHCs, and two critical access hospitals (CAH) in Washington County
- Industry leaders, such as Maine Quality Counts and Hanley Leadership
- Regulators, including Maine’s Department of Health and Human Services (DHHS) and the Health Resource Service Agency-Bureau of Primary Health Care in Washington, D.C.
EHC’s Community Circle program was additionally highlighted as an “up-and-coming” innovation in the 2013 Harvard Pilgrim Annual Report.
EHC currently convenes three focused Community Circles: the Integrated Behavioral Health Community Circle, the Gay/Straight/Transgender Alliances Community Circle, and the Caregivers/Palliative Care Community Circle.
Integrated Behavioral Health Community Circle
Spurred by health outcome data and the desire of providers to improve their patients’ health and wellness, EHC developed a plan for an Integrated Behavioral Health (IBH) Community Circle. The initial IBH Circle convened in June 2011, with a primary care provider and a behavioral healthcare provider co-leading the discussion among organizations that typically did not converse about integrating care. The leaders established an aim statement: “To improve the system of healthcare delivery in Washington County for patients and loved ones affected by mental illness.” In response to the growing opioid addiction epidemic in our county, the Circle expanded its aim to include those affected by substance abuse.
The Circle has met every six weeks since then at a central location in one of our county’s CAHs. More than 80 voices have contributed to the conversation, representing many sectors of the community: medical providers, behavioral health providers, peers, parents and loved ones of those affected by mental illness or substance abuse, faith-based organizations, educators, state legislators, state DHHS employees, university faculty, medical students, hospitals, law enforcement, local jail officers, patient advocates, National Alliance on Mental Illness (NAMI) Maine, veterans, teens, and others.
Outcomes of the IBH Community Circle include:
- Strong relationships and trust among organizations providing care (i.e., hospitals and primary care and behavioral health practices) and services (i.e., Downeast Correctional Facility, DHHS, NAMI Maine)
- Articles in the local paper highlighting mental illness, substance abuse, and the presence of shame
-
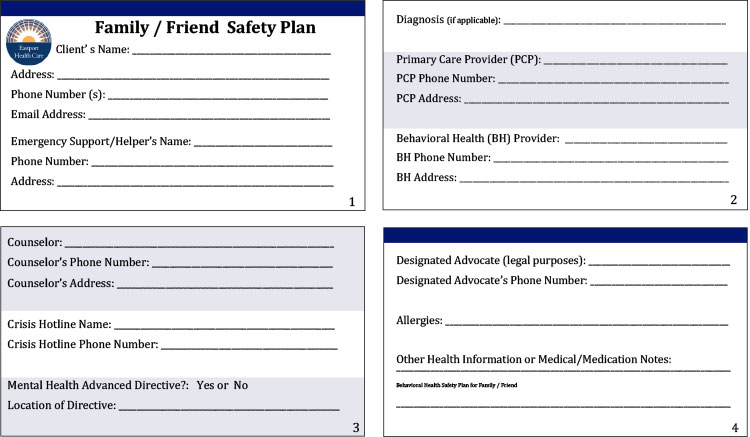
Figure 1. The Family/Friend Safety Card is a support tool for caregivers and loved ones of those affected with mental illness or dual-diagnosis substance abuse. The card ensures that relevant information is available quickly, in one place, should a crisis occur and emergent stabilizing care is necessary. It also helps with providing key information for timely coordination of care. Care and discharge planners are especially thankful to receive this information. The card is printed on two sides of one long strip. It folds in half to become approximately the size and shape of a standard business card. - Development and implementation of a patient safety card (Figure 1)
- Educating and promoting the use of Maine’s Mental Health Advance Directive, or MHAD (Maine is one of 14 states that have a MHAD)
- Education for Maine state legislators about Community Circles (and the IBH Circle in particular) through presentations to the DHHS sub-committee and the development of an annual event, “Bright Spots in Health Care in Washington County”
- NAMI sponsorship of a monthly support group and countywide training to ensure first responders across the healthcare system have an understanding of mental illness