Clinical Documentation: More than a Cumbersome Chore
January / February 2010
![]()
Clinical Documentation:
More than a Cumbersome Chore
“Charting” is often viewed by nurses as a necessary evil. Sure, deep down most nurses know that the exercise is essential — and that regulatory bodies such as the Joint Commission, National Quality Forum, and Centers for Medicare & Medicaid Services are looking for the clinical documentation that illustrates that care is being delivered in line with a set of established standards. And, in the end, such oversight is good for patient safety and quality care.
But in the day-to-day world of nursing, performing clinical documentation duties — the paperwork that so many nurses dread — often feels like an intrusive burden that simply eats up valuable time, those precious minutes and hours that could be better spent directly interacting with patients. And, the connection to quality and patient safety sometimes becomes obscure amidst the more immediate requirements associated with delivering high quality care.
The Opportunity
At Medical Center Hospital (MCH), Odessa, Texas, as we transitioned from paper medical records to an electronic medical records system, we decided to seize upon the opportunity to make clinical documentation more than just an obligatory chore — but an activity that nurses truly embrace as a quality and patient safety exercise.
Recognizing the potential benefits associated with electronic record keeping is what initially put us on the path toward improved clinical documentation. Certainly with electronic tools, clinical documentation could become a central part of the patient care process, performed as a routine duty at the patient bedside, not as an afterthought. In addition, electronic charting leads to better documentation because systems can provide tools that inhibit inconsistencies in documentation and facilitate 100% compliance of all required elements of clinical documentation.
The challenge? Finding a way to best leverage technology in an effort to improve clinical documentation while, at the same time, truly enhancing the quality of care and patient safety.
Leaders at the hospital formed a multidisciplinary team consisting of representatives from both nursing and information technology to address the challenge. The team examined how to leverage information technology with respect to making clinical documentation more meaningful and efficient for nurses. Through this analysis, the team came up with the following set of guidelines for the selection and implementation of the technology:
- Priority is given to applications/equipment that allow the healthcare provider to function at the bedside.
- Solutions to workflow issues will be addressed by modifying work practices, not customizing software products.
- Interdisciplinary communication and collaboration is valued.
- Hardware selections will be varied and determined by the end user.
- Location of supplies and equipment will be standardized on each patient care unit.
- In the balance between patient safety and efficiency, priority will be given to patient safety.
Like other providers, we had to ensure that we had the documentation processes in place that would help us meet The Joint Commission and other regulatory expectations. Getting our documentation efforts up to speed emerged as an even more pressing priority as The Joint Commission now conducts compliance audits without notice, whereas previously the accrediting organization would forewarn healthcare providers before conducting an inspection.
To address the challenge, we worked with an outside clinical consulting service to optimize clinical performance through process redesign, standardization and change management.
To start, we zeroed in on some common problem areas such as patient assessments, pain, and restraints documentation. The review helped us pinpoint if we had house-wide documentation issues or if certain departments or staff members were struggling in certain areas.
In addition to improving areas where our documentation efforts fell short, we also set out to meet the following three goals:
- Improve clinical documentation practices to more completely meet regulatory requirements.
- Make clinical documentation more efficient for caregivers.
- Elevate clinical documentation to a practice that enables clinicians to enhance quality of care and patient safety.
To address this multi-faceted challenge, consultants conducted a 2-day, in-depth, on-site analysis focused on the documentation compliance issues such as the timely receipt of restraint orders, tracking of required daily assessments, screening of admissions, pain management, and verification of vaccine administrations. The assessment uncovered various opportunities, including screen design that didn’t align with clinical workflow and priorities, differences in interpretation of actions that were compliant, difficulty determining compliance with patient online documentation, and retrospective sampling that did not provide a clear picture of facility performance.
Such problems were leading to incomplete clinical documentation, a common problem at many hospitals. In fact, a study published in the Journal of the American Medical Association, suggests that 14% of patient charts are missing critical patient information and, in many of these cases, the missing information could adversely affect care (Smith et al., 2005).
The Fix
With the problems identified, we then had to work on coming up with solutions. Our most important revelation: The analysis showed that the hospital needed to change the documentation process from a retrospective chore to a real-time proactive exercise. In addition, we needed to ensure that our electronic system would prompt nurses to document consistently.
Of course, the fact that our organization is using an electronic medical records system makes it possible to perform real-time charting at the point of care. An electronic medical records system, however, is not a panacea. Instead, organizations such as ours have to develop and implement systems that will encourage clinicians to properly use electronic tools to accurately document at the point of care.
To move the caregivers in our organization in this direction, the consultants utilized the established multidisciplinary team consisting of representatives from both nursing and information technology to prioritize and build retrospective and prospective documentation monitoring tools.
With guidelines in place for the use of electronic charting, hospital leaders also focused on finding ways to address specific clinical documentation issues — from the timely receipt of restraint orders to the tracking of required daily assessments to the screening of all admissions to determine vaccine administration.
Consultants specifically worked with nursing, informatics, and performance improvement staff to better leverage existing technologies. For example, they taught nurses and managers to use reports to proactively track and increase documentation compliance with the comprehensive suite of clinical solutions that we have in place to improve patient care.
In addition, the consultants worked with staff to:
- Conduct a comprehensive review and update related policies.
- Clarify performance expectations and create accountability tools.
- Align electronic documentation with clinical standards.
- Configure reports to enable nurses, charge nurses, and unit directors to identify and address documentation compliance prior to the end of the shift
- Establish retrospective executive tracking and reporting mechanisms.
- Train 53 charge nurses and unit directors on the new process.
The Results
By adopting prospective end-of-shift reports for charge nurses and retrospective reports for clinical executives, MCH has improved compliance with clinical documentation standards. At the same time, we have transformed documentation into a value-laden activity that truly improves care.
After just one month, completed assessments rose from just 55% to about 85%. In addition, the hospital has experienced a 65% improvement in completing admission assessments per policy and a 67% improvement for completing required vaccine screening. Perhaps most telling, no clinical documentation issues were cited by The Joint Commission during a recent assessment.
Many times, performance improvement is temporary, as an organization shifts its focus to other needs. The tools and processes adopted by MCH have enabled MCH not only to maintain these gains, but actually continue to improve, even as the facility tackles other clinical initiatives. From January of 2009 to June of 2009, compliance with admission assessment has continued to improve (Figure 1, page 38).
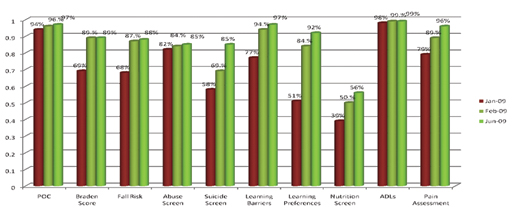
Figure 1: Admission Assessment Charting Compliance
(click here to view a larger version in another window)
Perhaps most importantly, the new clinical documentation process is enabling nurses to spend more time at the bedside. All too often, nurses are reluctant to begin electronic charting at the patient’s bedside because they fear the exercise will interfere with care. However, with electronic charting in place at MCH, nurses are now spending 10% more time in direct patient care activities (Mathur et al., 2008).
The real-time documentation also helps to improve care on the spot. For example, when nurses document a patient’s pain score or the Braden scale at the point of care, the nurse is then more likely to immediately address the patient’s issue, and, therefore, deliver improved care. The very fact that they are documenting on the spot makes the nurse more aware of the patient’s pain — and, in turn, makes them more accountable in terms of addressing the issue. Because the nurses know that the score is being captured and reviewed daily, they are more likely to take a more proactive tact when pain is present.
The availability of data also provides clinical managers the ability to proactively identify target areas of improvement. For example, the data now reveals if a specific unit or staff member needs to change practice to improve quality or comply with regulations. As a result, managers can develop focused interventions to bring about the desired improvements before the end of the nursing shift.
What’s more, real-time clinical documentation helps to improve care by enhancing communication among caregivers. With real-time charting, all clinicians can consult the chart to get an accurate up-to-the-minute assessment of patient care needs. As such, nurses can be more aware of patient safety issues such as fall risks. In addition, the real time documentation helps when nurses need to communicate with doctors about a patient’s care and needs. With end-of-shift paper documentation, hand-offs did not work out nearly as well. Missing clinical information, as a matter of fact, is associated with 15.6% of all primary care clinical errors (Stiell et al., 2003). And, a recent study of Canadian emergency department physicians reported that 15.3% of visits had important information missing at the time of the encounter, which could lead to patient harm (“Toxic Cascades,” 2001).
|
Medical Center Hospital in Odessa, Texas, worked with McKesson’s Clinical Consulting Services, an offering that optimizes clinical product performance through process redesign, standardization, and change management, to enhance clinical documentation by improving compliance with documentation standards, decreasing the variability of care, reducing medication errors, and accelerating return on investment. The hospital also utilizes McKesson’s comprehensive suite of clinical solutions. |
With these improvements in assessment, documentation, and communication, we are beginning to see care improvements. For example, we have experienced a reduction in pressure ulcers. By doing a better job with the assessments, we can get patients the care they need — and avert the development of pressure ulcers.
Such improvements also lead to a healthier bottom-line. For example, a drop in pressure ulcers will lead to decreased costs — especially as hospitals are no longer reimbursed for pressure ulcers that develop while patients are in their care, according to a Centers for Medicare and Medicaid rule that went into effect in October 2008. And, costs to treat such infections can add up quickly. According to CMS research, the average pressure ulcer costs about $40,381 to treat (Shraag, 2007). Staff members also more efficiently track completion of required documentation. Cost avoidance for this initiative has resulted in a two-to-one return on investment. The hospital would need three FTEs to attempt to conduct 100% manual chart reviews. By averting this cost, the hospital saves about $190,000 per year.
By realizing the power of electronic documentation, then engaging in a dedicated effort to figure out how to best leverage automated tools, Medical Center Hospital has been able to turn clinical documentation into an activity that not only helps us meet regulatory requirements more completely and efficiently, but also helps us to deliver better care to the community and to do so in a more cost efficient manner.
Marlene McAlister is the CNO and Sherrill Rhodes is director of performance improvement at Medical Center Hospital. The 362-bed hospital in Odessa, Texas, employs 1,600 staff members and has 275 active physicians. Rhodes may be contacted at SRhodes@echd.org.
References