ASQ Healthcare Division Newsletter
March / April 2010
Applied Operations Management Concepts Lead to ED Operational Improvement
There is a significant body of knowledge, taken from other industries and effectively applied to emergency department (ED) flow, that is beginning to coalesce into a conceptual framework to approach ED operations. When combined effectively, the following operations management concepts create the ideal framework to drive your ED towards an operational excellence approaching the most successful companies in the world, even though it is one of the most challenging service environments in which to innovate and improve.
Lean Healthcare
What is Lean Healthcare? Lean Healthcare represents the evolution and diffusion of Lean applications in other industries into healthcare. Lean Healthcare can be characterized as following key components:
- Creating patient value
- Eliminating waste
- Promoting flow
- Continuous improvement
- Developing people
Creating Patient Value
Lean Healthcare seeks to enhance patient value by creating and defining patient value streams, or groups of patients that follow the same basic steps throughout their visit. All of the activities in a patient process can be classified as value-added or non-value-added. Value-added activities are those steps that move the patient closer to wellness, to services that they desire, and that are done right the first time. Non value-added activities are those steps that do not create patient value and that they do not want or desire. One way to zero-in on non-value-added activities is to describe them in terms of the classic eight Lean forms of waste that are present in every process.
- Transportation
- Movement
- Inventory
- Waiting
- Over processing
- Over production
- Defects
- Human creativity
The goal of any Lean improvement effort is to create value and eliminate waste within processes, continually driving up the amount of value-added activity relative to the amount of non-value-added activity, increasing the “value-added ratio.”
Promoting Flow in the Context of Queuing Theory
Because healthcare is a highly specialized service industry with high degrees of variation, flow must be managed much more intensely than in manufacturing. This is done employing queuing theory and the theory of constraints.
Queuing theory is the mathematical study of waiting lines. It was developed to provide models to predict the behavior of systems that attempt to provide service for randomly arising arrivals, rather than for constant or scheduled arrivals. By understanding the arrival rate and service rate of all of the critical servers in the ED (physicians, nurses, and beds), and how they react under different situations, one can begin to design a system that is very responsive from a service perspective.
An important consideration when discussing queuing theory is the relationship between service responsiveness and server utilization. In general, as the amount of variation and the utilization of servers increases, the waiting increases at a disproportional rate (exponentially). When systems with high degrees of variation are at high utilization rates, they tend to go bad fast!
In order to improve queuing systems, we can try to affect the amount of variation, the arrival rate, the service rate, the arrangement of servers, or the queue discipline (or the way the system prioritizes various arriving patients).
The Theory of Constraints
The Theory of Constraints was described by Eli Goldratt over 20 years ago. His theory states that improving bottleneck resources (perhaps through applying Lean principles) is the only way to enhance throughput. Working on non-bottleneck resources is a mirage. An organization’s goal is to aggressively manage its system’s constraints, repeatedly removing the constraint that represents the greatest relative bottleneck. Attending to bottlenecks in this fashion is the most efficient method of accelerated organizational improvement.
Continuous Improvement and Developing People
Perhaps the most important aspect of Lean healthcare is its relentless pursuit of perfection. This core principle permeates most lean organizations and shows in the way it approaches problem solving and the development of its people. Lean organizations place front line workers in control of improving the system, as these people are the only ones who have the answers. Lean organizations empower their staff members by teaching them tools to help them improve their workplace. These tools, as spokes, with the hub Plan-Do-Check-Act (PDCA), create the wheel of continuous improvement.
Swedish Medical Center – Applied Operations Management
Swedish Medical Center is a great example of all of these concepts coming together to create an exceptional multi-hospital dramatic operations redesign across four emergency departments. After an intense 5-day Lean ED education session involving physicians, nurses, improvement engineers, administration, and other support staff, in which they learned all of these concepts in the context of an ED operational transformation, Swedish set out to do just that—transform their care delivery model. They had a great deal of work to do, however, with long waits to see providers and long lengths of stay in 3 of 4 of their hospitals and widespread diversion. In January of 2009, Cherry Hill and First Hill combined had 130 diversion hours (Figure 1). In March of 2009, First Hill had a door-to-doc time of 55 minutes. Length of stay for treat and released (T&R) patients was 3 hours and 11 minutes, and treat and admit (T&A) was 4 hours and 6 minutes.
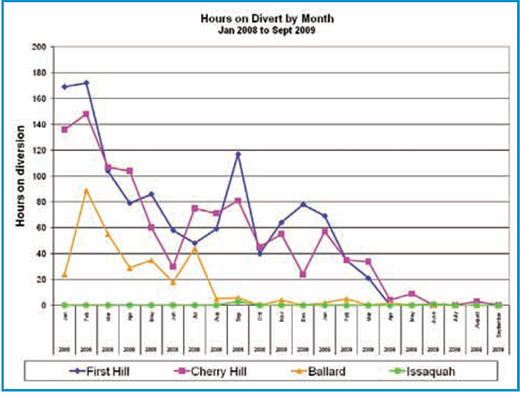
Figure 1: Diversion hours at Swedish from Jan 2008 to Sept 2009
By April, only 3 months later, Swedish was successful in virtually eliminating diversion across all of its facilities. In fact, from April to December, Swedish had less than 20 total diversion hours across all of their hospitals!
They did this by applying lean concepts, focusing on creating patient value and eliminating waste. By leveraging queuing theory and applying the theory of constraints, they were able to reduce variation in the patient experience by transforming the way they treat certain patient streams, primarily focusing on the T&R patient population. In doing so, they were able to dramatically reduce LOS; one year later, First Hill had reduced its T&R LOS from 3 hours and 11 minutes down to 2 hours and 37 minutes (a 17% reduction), and reduced its T&A LOS from 4 hours and 6 minutes down to 3 hours and 35 minutes (13% reduction). Most importantly, they reduced their door- to- doc time from 55 minutes down to a low of 32 minutes in December of 2009 (41% reduction).
Most importantly, Swedish did this with just education, no pricey consultants who come in and recommend changes that may or may not work. By learning these critical concepts and then, in the true lean spirit, becoming a community of scientists, Swedish has developed their own internal, front-line capacity for operational improvement and innovation. They are now spreading this knowledge upward throughout their hospitals to further improve patient care in areas remote from the ED.
Lean thinking can turn that weakness into an opportunity to examine an innovative approach to ED operations improvement. Our hope is that EDs across the country begin to think within a Lean framework, even if they don’t call it Lean. If we all adhere to the fundamental principles described above as Swedish Medical Center has been able to do, we will be able to continuously improve the provision of emergency medicine for our patients and staff.
References
Ozcan, Y. A. (2009). Quantitative methods in health care management: Techniques and applications (2nd ed.). San Francisco: Jossey-Bass.
HCD Recognizes Dr. Eitel for His Leadership
Inevitably in life, there comes a time when one must move on. Regrettably for the HCD, that time has come for David Eitel, MD, who has led the HCD through a year during which his father passed away; he wrote a book, Emergency Department Throughput; taught a graduate course in process improvement, and resumed the practice of emergency medicine after a long hiatus. Dave has decided for personal reasons not to complete the second year of his two-year term as HCD Chair.
During his watch, the HCD generated the ASQ White Paper on Healthcare Reform and two ASQ comments on aspects of the Health IT legislation. The Division also got serious about a new healthcare quality certification. Dave was also the architect of our partnership with the Society for Health Systems in the Building Better Healthcare Systems conference held in February.
Individually and collectively, the Healthcare Division owes a great debt to Dave for his leadership and for the contributions he has made to strengthen and grow the HDC in troubled economic times. His formula for this was simple: by creating and delivering real value to our Division members, we can ensure the Division’s growth and effectiveness!