|
 |
|
July / September 2004
Computerized Physician Order Entry
CPOE at a
Community Hospital:
First Steps
Maggie Lohnes, RN, CPHIMS, FHIMSS
The crescendo of recommendations from regulatory, clinical, payer, and purchaser groups touting applications such as computerized physician order entry (CPOE) as solutions to unacceptable error rates is hard to ignore. Success at government and academic hospitals whose physician staff are primarily employees with a single practice site has been well documented. Community hospitals, serving private practitioners who often practice at multiple facilities as well as their own offices, have been slow to adopt these technologies, stymied by a unique set of obstacles.
This is the first in a series of reports that will follow one community hospital's progress as it advances its computer functionality toward the goal of improved patient care. Implementers at Huntington Hospital have chosen an open approach, a demonstration project of sorts, in an effort to take advantage of the brain trust in the healthcare information technology community and avoid the pitfalls of brave early adopters. Readers are encouraged to comment on prospective plans and provide input from experience, with the goal of enjoying mutual pride in the ultimate success.
Strategic Plan for Information Technology
Huntington Hospital, a 525-bed not-for-profit tertiary care community hospital, was established in Pasadena, California, in 1892; its mission is simply to excel at the delivery of healthcare to its community. Taking a cue from its namesake — Henry Huntington, the tycoon who brought the Pacific Electric Trains to Los Angeles — Huntington Hospital has long embraced technology for the improvement of its services. Healthcare information systems are welcomed for their positive impact on quality, patient safety, and operational efficiency.
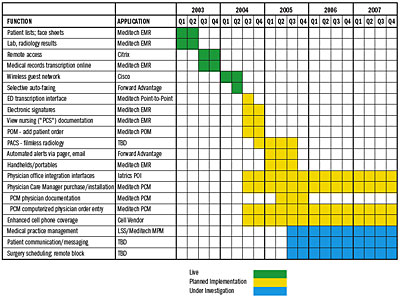
Huntington Hospital's experience with healthcare information systems follows that of the typical community hospital, first acquiring financial systems, followed by patient tracking, results reporting, and patient billing systems. The hospital survived Y2K unscathed due to an exhaustive effort to reprogram its unsupported legacy systems with compliant code, leaving functional, though perfunctory, automation. Functionality for physicians consisted of printing patient lists and locating lab results.
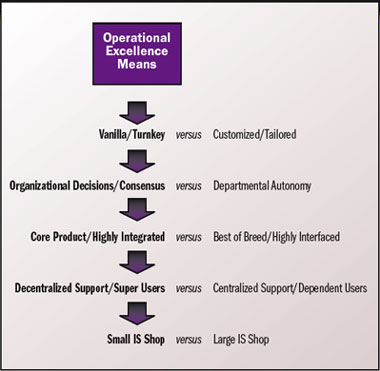
With Y2K behind it, Huntington Hospital looked ahead with the development of an aggressive long-term information technology strategic plan. Huntington Hospital's information technology strategy is aligned with its overall business strategy emphasizing operational excellence�organizing to deliver high-quality service at a competitive price. Figure 1 (page 14) illustrates the key operational pillar of Huntington's overall strategic premise of "market indispensability" as approved by its Board, and the technical strategy that supports it. It is this tenet that drives and guides the information technology plan at Huntington Hospital.
|
|
|
 |










|
 |