Red Flags that Represent Credible Threats to Patient Safety
March/April 2013
![]()
ISMP
Red Flags that Represent Credible Threats to Patient Safety
Disruptive behaviors, intimidation in the workplace, and a culture of disrespect among healthcare professionals have repeatedly surfaced as significant barriers to patient safety. The hierarchical nature of patient care and the autonomy with which healthcare professionals have been taught to practice set the stage for a culture that does not respond well to even the slightest queries about possible problems with patient care, particularly from subordinates. It’s clear that such a culture needs to be repaired, and many healthcare organizations are working to address disrespectful behavior, staff reluctance to speak up about risks and errors, and blatant disregard of expressed concerns. However, there’s a less obvious but no less dangerous risk related to the culture that often goes unnoticed until a serious adverse event happens: staff do speak up about potential concerns, but they are too easily convinced that their concerns are unfounded.
When a person voices a concern, there’s often no disruptive, disrespectful, or obvious intimidating behavior involved per se, but rather an explanation from competent practitioners that dispels the initial concern too quickly, before it has been given sufficient consideration. A pharmacist reassures a technician that the compounding directions are correct when questioned about an unusual volume of ingredients; a pharmacist assures the nurse that the strength of the infusion is correct when questioned about the final volume; a nurse reassures a patient that the medication is correct when questioned about its appearance; a physician convinces a pharmacist that the prescribed dose is correct when questioned because it differs from a protocol—these are all-too-frequent examples that have led to fatal adverse drug events. Those who questioned the patients’ care were easily convinced that others knew more than they did, particularly if the provider who was questioned had an otherwise stellar reputation.
Is this a form of intimidation? Perhaps, but it is more akin to a logical deference to expertise, meaning it is natural and often reasonable for people to defer final judgment to those who they perceive to be more “qualified.” If the person voicing the concern was reluctant to pursue it, avoided or backed down from the conversation, or felt the provider was not listening, workplace intimidation may play a role. But this is not always the case. Instead, the issue may be that the person questioning the patient’s care has been easily convinced that their concern is unfounded, and the person being questioned has not perceived the voiced concern as a possible, credible patient threat. Neither possesses a required element to safeguard patients: an appropriately high index of suspicion for errors. A low index of suspicion is particularly problematic in a healthcare system that already is reluctant to acknowledge human error or value the contributions from every person, regardless of rank, who interacts with the patient.
An index of suspicion is defined as “awareness and concern for potentially serious underlying and unseen injuries or illness” (American Academy of Orthopedic Surgeons, 2010). Suspicion is defined as “the act or an instance of suspecting something wrong without proof or on very slight evidence, or a state of mental uneasiness and uncertainty” (Merriam-Webster). A high index of suspicion requires consideration of a large differential so that a serious possibility is not accidentally discounted; a potential medical error should always be considered one of the possibilities. An appropriately high index of suspicion should lead a person with a concern to pursue it until it’s proven to not be a credible patient threat, even when met with opposition from experts. It should also prompt the provider to be responsive to voiced concerns and to initiate a suitable investigation to determine if there is a credible threat to the patient.
ISMP has previously discussed the need to maintain a high index of suspicion for errors, including in the March 9, 2006, newsletter about mindfulness, a defining characteristic of high-reliability organizations (HROs). Mindfulness refers to the deep and chronic sense of unease and preoccupation with failure that arises from admitting the possibility of error, even with well-designed, stable processes (ISMP, 2006). People in HROs worry about system failures and human errors. They ask, “What will happen when an error occurs?” not “What will happen if an error occurs?” Like healthcare, HROs are hierarchical, but position and experience do not necessarily dictate who is an important contributor or decision maker. They are wary of complacency and naturally suspicious, so they expect people to speak up about any concerns they may have. Their high index of suspicion is a predominant factor in achieving laudable safety records.
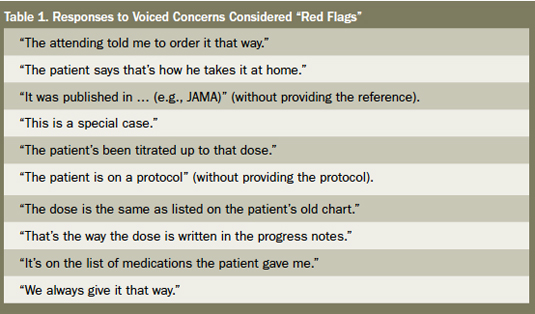
To improve patient safety, healthcare needs to raise the index of suspicion for errors, always anticipating and investigating the possibility when any person, regardless of experience or position, voices concern or when patients are not responding to treatment as anticipated. Functional patient care teams, in which every person’s perspective, skills, knowledge, and observations are considered important and worthy of mention and investigation, must be developed. Staff members need to be mentored on how to resolve potential concerns and to trust in their own experiences to augment the expertise of others. All healthcare practitioners need to encourage and be receptive to staff who ask questions, even if staff just have a sense that “something” is wrong or can’t articulate the concern well. When concerns are met with quick answers that initially appear to be “evidence” of safety, caution is recommended. Thirteen years ago, our colleague, Timothy Lesar, PharmD, of Albany Medical Center in Albany, New York, allowed us to publish a list of phrases he called “magic words” which have been repeatedly offered in explanation to voiced concerns and erroneously accepted as “evidence” (Table 1; ISMP, 1999). No doubt, these still ring true today, along with many others. Such phrases should be viewed as “red flags” that require more reliable answers and actual proof.
ISMP is not discounting the fact that intimidation may play a role in a reluctance to speak up about possible concerns and a tendency to be easily convinced that a concern is unfounded. We also do not discount the extraordinary courage it may take for many to step up to these conversations. However, healthcare practitioners also need to acknowledge that a natural deference to expertise can lead to unintended complacency and tolerance of risk that goes unchallenged. To combat that, all who interact with patients must reduce their tolerance of risk and raise their index of suspicion of errors.
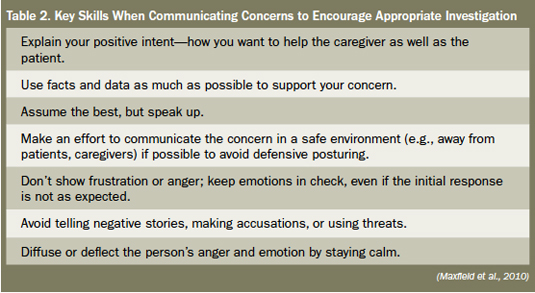
A 2010 study conducted by VitalSmarts, the Association of periOperative Registered Nurses (AORN), and the American Association of Critical-Care Nurses (AACN), offers insight into the key skills that can encourage an appropriate response to voiced concerns (Maxfield et al., 2010). These skills are summarized in Table 2. The study concludes that there is cause for optimism—concerns are being voiced nearly three times more often than just 5 years ago. Healthcare practitioners need to ensure that these concerns are not only raised but also properly investigated and addressed. You can be sure that those involved in serious errors wish that they had taken the opportunity to do just that.
This column was prepared by the Institute for Safe Medication Practices (ISMP), an independent, nonprofit charitable organization dedicated entirely to medication error prevention and safe medication use. Any reports described in this column were received through the ISMP Medication Errors Reporting Program. Errors, close calls, or hazardous conditions may be reported online at www.ismp.org or by calling 800-FAIL-SAFE (800-324-5723). ISMP is a federally certified patient safety organization (PSO), providing legal protection and confidentiality for patient safety data and error reports it receives. Visit www.ismp.org for more information on ISMP’s medication safety newsletters and other risk reduction tools. This article appeared originally in the July 26, 2012, issue of the ISMP Medication Safety Alert!
References